Is your newborn making abnormal sounds while breathing? Watch out, for it may be a case of Laryngomalacia that is the actual cause. Read and know all about the causes, symptoms, diagnosis and treatment options for this disorder.
Laryngomalacia Definition
Page Contents
- 1 Laryngomalacia Definition
- 2 Laryngomalacia ICD9 Code
- 3 Who Suffers from Laryngomalacia?
- 4 Laryngomalacia Symptoms
- 5 Laryngomalacia Causes
- 6 Laryngomalacia Diagnosis
- 7 Laryngomalacia Treatment
- 8 Laryngomalacia Complications
- 9 Laryngomalacia Prevention
- 10 Laryngomalacia Prognosis
- 11 Laryngomalacia and Acid Reflux
It is a congenital malformation of the laryngeal cartilage, meaning it is present at birth. However, it is not a serious condition in the majority of cases.
This anomaly of the larynx is also referred to as “Soft Voice Box” or “Soft Larynx.”
Laryngomalacia ICD9 Code
The ICD9 Code for this disease is 748.3.
Who Suffers from Laryngomalacia?
The condition is quite common in infants and young children although it may also arise in some adults. Older adults, particularly those suffering from weakened throat muscles due to neuromuscular disorders, can suffer from this disease. However, the disorder is much more common in infants.
Laryngomalacia Symptoms
A person affected by this disorder tends to make abnormal noises, especially a whistling sound (stridor) while breathing. Stridor refers to a high-pitched noise that can be heard when a child breathes in (inspires). It can sound like snoring through a congested nose or high-pitched squeaking. In some cases, the sound is audible to anyone present near the sufferer. In the rest of cases, the noise can be heard only with the help of a stethoscope.
Picture 1 – Laryngomalacia
In some infants, the area at the throat base can be found to sink in with inspiration. In others, the region under the diaphragm is observed to drop.
While stridor is mainly audible during the inspiration of infants, it can also be heard at the time of expiration (breathing out). Some other features of the condition include:
- Alteration of stridor with activity, possibly improving when an infant cries severely
- Stridor generally getting less noisy when a child lies on the stomach
- Stridor turning worse in case of an upper respiratory infection
Around 60% infants born with this disease tend to experience its symptoms as early as in the first week of their life. The majority of the remaining infants exhibit its signs and symptoms by 5 weeks of age. The symptoms begin during the first 2 weeks after birth, generally at times when a baby is in distress, crying or lying down.
The signs of this disorder may appear similar to various other conditions or ailments. The disorder is also often confused with colic. In some cases, parents take affected babies to physicians with the belief that their child suffers from a lingering cold without any nasal discharge.
This condition is the most common cause of a disease known as Congenital Laryngeal Stridor. It is important for parents to consult a physician in case their child displays symptoms associated to Laryngomalacia.
Laryngomalacia Causes
The problem is caused due to the inward collapse of the softening tissue at the time of inhalation. The collapse occurs as the cartilage and the soft tissue around the larynx, or voice box, becomes too feeble to support the pressure of breath. The inward flapping of the tissue leads to an obstruction (blockage) of the airway.
The condition has not been associated with any particular gene. However, some evidences suggest that the condition might be inherited in certain cases. The disease has not been found to show any predilection for race.
Laryngomalacia Diagnosis
During diagnosis of the condition in infants, doctors are likely to ask about the problems experienced by babies. Apart from physical examination and an analysis of complete medical history, diagnostic measures may involve Flexible Laryngoscopy. This method may be used to determine the condition further. In this procedure, a physician may enter a flexible, lighted tube through the nose and deep down into the throat of a patient to view his or her voice box. It would help him find out if the affected individual is suffering from Laryngomalacia of mild, moderate or severe intensity. The severity of the disorder can help in determining an appropriate treatment plan for its sufferers.
This process is usually conducted in the office of an otolaryngologist. It is best performed when a suffering child is awake. If the condition is not conclusively detected in an office setting, the affected infant may have to undergo general anesthesia. The process may be carried out in a more careful manner to study the airway under the voicebox and look for other disorders that may result in stridor.
Laryngomalacia Treatment
The need for treatment is low as long as a baby develops normally, feeds well and gains weight at a normal rate. The disease usually shows an improvement by the time an infant is 1 ½ years of age and does not suffer from any long-term complications. In certain cases, the stridor can be noted until the baby turns at least 5 years old.
The case of each infant affected with this disorder is unique. A small percentage of Laryngomalacia sufferers develop acute respiratory problems that need medical and surgical interventions – usually within the first few weeks to months after birth.
Supraglottoplasty is the mainstay for surgical intervention in this disease. This operative process involves removal of the obstructing collapsing tissue with the aid of an endoscope. Tracheotomy is used only rarely; it is put to practice only in cases where supraglottoplasty fails to bring about an improvement and when patients suffer from more than one medical co-morbidities.
Medications
Patients suffering from Laryngopharyngeal reflux (LPR) and Gastroesophageal Reflux Disease (GERD) experience an improvement in their symptoms with the help of Acid Suppression Therapy. Gastric contents can lead to a swelling or inflammation in the posterior section of the larynx and make it flop even more into the airway. Therefore, treatment of GERD can help in curing Laryngomalacia. GERD is noted in 65-100% of all cases of this disorder.
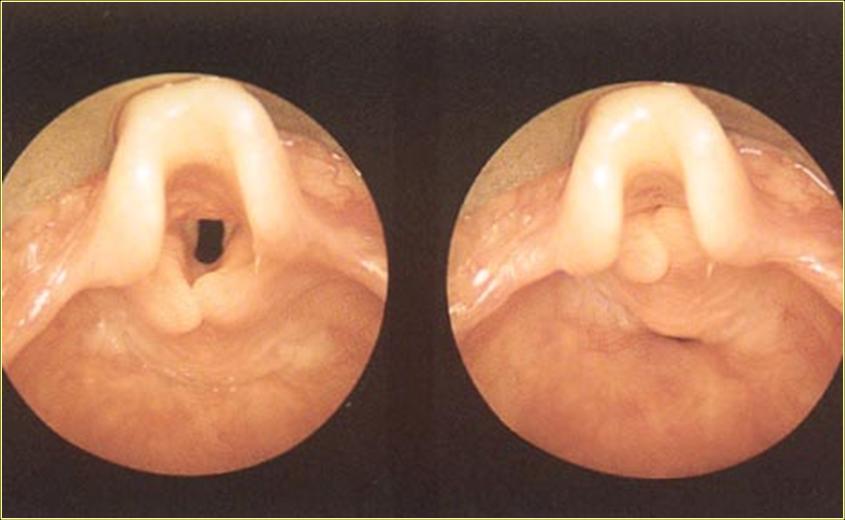
Picture 2 – Laryngomalacia Image
It should be noted that drug therapy is not regarded as a part of standard therapy for this disorder.
Surgery
Operative measures are considered when a patient cannot breathe or eat normally. Tracheotomy is a surgical process that involves making an opening in the neck to result in a direct airway to the windpipe. Laryngoplasty is an alternate measure that may be conducted to strengthen the support structures (tissues and cartilage) surrounding the voice box and ablate any extra tissue surrounding the larynx.
Inpatient care is not required unless an affected baby suffers from medically significant cases of apnea or hypoxemia.
In case of Laryngomalacia in infants, the supraglottic larynx (or the section over the vocal cords) is curled tightly. A short band known as aryepiglottic fold is used to hold the cartilage shield tightly in the front to the movable cartilage in the arytenoids – the posterior section of the larynx. The bands help the epiglottis to get curled automatically on itself.
Laryngomalacia Complications
The complications associated with this disease include:
- Apnea
- Poor oxygenation that needs supplemental oxygen therapy
- Alveolar hypoventilation that requires surgery or positive pressure ventilation
- Elevated risk of GERD (Gastroesophageal Reflux Disease)
- Pulmonary hypertension
It is only in rare circumstances that affected infants suffer from serious, life-threatening obstruction of the airways. Most patients are found to suffer from stridor and free from more severe symptoms like respiratory difficulties (Dyspnea).
Laryngomalacia Prevention
The condition cannot be prevented. As the disease does not run in individuals of the same family (meaning no hereditary association has not been conclusively proved), it is difficult to know which couple is likely to give birth to a child with this condition.
Laryngomalacia Prognosis
The condition usually gets worse over the first year of the life of an infant, as the baby begins to breathe in and out more vigorously. In the majority of cases, the condition is harmless and heals on its own with time – without the need for any medical intervention. The stridor tends to get worse as a baby grows; only to disappear slowly as the cartilage and the tissue begins to get stronger and support the larynx.
It is only in rare cases that the condition may cause as much hypoventilation or hypoxemia as to interfere with normal development of affected infants. In acute cases, particularly those connected with GERD, problems with feeding (such as gagging or choking) may arise.
In over 90% cases of this disease, time is the only cure. In almost all cases, the noises go away and the lesions slowly improve by the time patients are around 2 years old.
Laryngomalacia and Acid Reflux
Laryngomalacia is often associated with acid reflux. The resting and eating positions of sufferers might require alteration for the reflux to be avoided. In case the reflux is acute enough to bring stomach acid to the larynx, patients may suffer from inflammation and worsened cases of stridor at the time of inhaling. Physicians may prescribe medication for treating the reflux if repositioning fails to bring about any improvement in the condition of affected individuals.
As aforesaid, Laryngomalacia is a non-serious condition that usually resolves after a period of time. However, it is safe to consult a healthcare professional and opt for proper treatment in case medical cure is recommended.
References:
http://emedicine.medscape.com/article/1002527-overview
http://en.wikipedia.org/wiki/Laryngomalacia
http://www.choa.org/Child-Health-Glossary/L/LA/Laryngomalacia
http://www.wisegeek.com/what-is-laryngomalacia.htm
